

What is paediatric sleep apnoea?
Sleep apnoea is a lack of adequate oxygen supply to the brain. This is caused by an obstruction to airflow when breathing. In kids, this is most commonly due to enlarged tonsils and adenoids.
What causes enlargement of tonsils and adenoids in kids with sleep apnoea?
No one knows, but it appears to be genetic. We often see that more than one child in a family has sleep apneoa so it may be worth screening all the kids if you see symptoms develop. This is particularly true if there are cousins or parents or grandparents with sleep apnoea.
How does sleep apnoea differ in kids compared to adults?
Adult sleep apnoea is more likely to be due to obesity, alcohol and smoking. Adults can pause in their breathing for up to 10 seconds before their blood oxygen supply to the brain drops, whereas kids can generally only tolerate a 1-2 second pause.
Sleep apnoea causes adults to become tired and forgetful in the daytime. Sleep apnoea can also cause kids to be tired, but more often it causes bad behaviour. They will often be cranky. Because the kids are not refreshed by their sleep, their learning is affected. In little kids, you see speech problems as speech is their greatest learning task.
Older kids can be anxious and irritable due to sleep apnoea, but in this group we also see dental changes.

How does a blocked airway affect the teeth?
If a child does not breathe through the nose, the teeth and jaw can alter from the normal position, leading to expensive orthodontic work later.
A blocked nose which may be due to enlarged adenoids, can cause a high arched palate. As the palate rises, the teeth in the upper jaw become crowded.
As the crowded teeth angle in or out it becomes a “crossbite”. With a constantly blocked nose, these kids breathe through their mouth. This leads to an overbite with the upper jaw coming forward compared to the lower jaw.

An “adenoid face” is long, with the mouth open and dark rings under the eyes. Sometimes allergy is part of the equation so it is worth a trial of Claratyne or Zyrtec to see if this helps the breathing through the nose.
What are the symptoms of paediatric sleep apnoea?
As mentioned above, there can be irritability , bad behaviour and poor speech development. The bad behaviour may be misdiagnosed as ADHD. Most people think sleep apnoea causes snoring but up to a third of kids with sleep apnoea don’t snore.
For those who do snore, watch for pauses in the breathing and choking noises as the kids re-establish their airway.
To stretch open the airway, kids will often sleep with their head and neck tilted right back. Their sleep is restless. If they are in your bed, they will kick all night. The restlessness is due to the brain signalling the oxygen supply is too low. Kids then try to find a better position. Sweating or even bedwetting at night can be due to similar causes. Sometimes the child wakes during the night.
At mealtimes you may notice that your child avoids bulky food such as meat, preferring slippery food such as cheese, yoghurt and milk. This is easier to swallow past the enlarged tonsils.
What is the treatment of paediatric sleep apnoea?
First see your local doctor and take an iphone video of your child sleeping. Your doctor will look at the child’s airway. Remember sleep apnoea is about airway obstruction and not recurrent tonsillitis, so your local doctor will look for enlarged tonsils as well as signs of nasal obstruction such as the high arched palate, crowded teeth, overbite.
Sometimes the tonsils don’t look too large, but the mouth or jaw is small, so even moderately sized tonsils crowd the airway.
If your local doctor is concerned, they will refer you to either an Ear Nose & Throat Surgeon or a Paediatric Sleep Specialist. A sleep study will be discussed, particularly if the diagnosis is uncertain.
The definitive treatment for paediatric sleep apnoea is removal of the tonsils and adenoids – called adenotonsillectomy.
What is a sleep study?
A sleep study involves a night in hospital. Your child’s oxygen level will be monitored as well as the heart rate and breathing rate. An arousal index will indicate how disrupted the sleep is.
These numbers all count towards the AHI or apnoea/hypopnoea index. Your doctor will decide whether this means surgery. The only alternative to surgery is a facemask where oxygen is delivered to the child under pressure to stop the low oxygen levels when sleeping.
What does adenotonsillectomy involve?
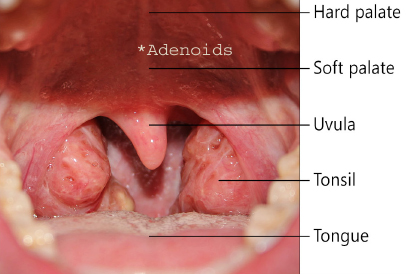
Three percent of Australian kids have sleep apneoa. It is now the most common reason for kids to have their tonsils removed. The tonsils lie at the back of the throat, next to the tongue. The adenoid is behind the uvula (part of the soft palate, see diagram).
Tonsils and adenoids are lymph glands. We have 120 lymph glands in the head and neck to filter infection. Taking out 3, namely the tonsils and adenoids, does not create a problem with immunity. In fact, it may help, particularly if your child has a constant runny nose. Asthma and allergies in the nose also tend to do better if breathing is improved by removal of the adenoids.
The surgery is done under general anaesthetic. You will be there as your child breathes into a mask and falls asleep. Half an hour later you will be with them in the recovery ward as they wake up. Most kids eat within hours of surgery and up to a third of kids can go home on the day of surgery if they are eating well and their pain is under control.
What pain medicine is needed?
Regular Panadol is the best pain relief. Oxynorm (Oxycontin) can be added on top. Some hospitals suggest alternating Panadol with Nurofen. Nurofen however must be strictly avoided before the operation as it can increase the risk of bleeding at the time of surgery.
Most kids need about a week of pain relief. Two weeks at home, watching DVD’s and quiet behaviour is also important to reduce the risk of bleeding.
What should you expect after surgery?
Usually the breathing at night is so much quieter, even straight after surgery. Sometimes swelling causes mild snoring for 4-5 days. Kids now have a much deeper sleep at night. This can temporarily lead to REM rebound or dream sleep. The kids may have 1 or 2 nightmares as they have a rush of dream sleep. This usually settles after 2 weeks.
Even as early as 2-3 weeks following surgery parents notice their child is more settled in the daytime as their sleep is deeper and more refreshing.
By two months, parents say their kids are eating more, filling out and growing. This is due to the levels of growth hormone produced in the deep sleep cycle the child did not previously experience normally.
Parents who have seen one child benefit from the surgery are keen to have younger siblings treated as soon as they show signs of sleep apnoea. Mothers often request referrals.